Monovision and refractive surgery
Monovision is one of the resources that ophthalmologists use to correct distant and near vision in patients with refractive disorders (myopia, farsightedness y astigmatism) and older than 40 years, affected by Presbyopia or eyestrain.
Monovision and refractive surgery
Monovision is one of the resources that ophthalmologists use to correct distant and near vision in patients with refractive disorders (myopia, farsightedness y astigmatism) and older than 40 years, affected by Presbyopia or eyestrain.
What is monovision?
With the monovision basically what we do is to correctthrough refractive surgery, everything the graduation defect in the dominant eye, we neutralize it to obtain a good vision from afar y, in the non-dominant eye, we induce a discreet myopia so that you can focus on the objects closely, in this way, we get, looking with both eyes (binocular vision), that the patient can see far and near without using the glasses.
That said, some may think that using one eye for each vision is not the best way to solve problems, and they will not be far off if things are not done well.
When we reach the age of presbyopia, we all have a certain dominance of the eyes, a certain degree of monovision occurs physiologically. There is always one eye that sees better from afar (dominant) and the other eye from near (not dominant). The difference is small since otherwise we would lose one of the most important properties that the visual system has, that of seeing in relief, stereopsis, key to calculate distance or see 3D movies in the cinema.
When a patient asks us to remove the glasses, far and near, we have several options, from laser treatments on the cornea to refractive treatments with multifocal intraocular lenses. When we see that a multifocal lens is not the best solution for that case (see multifocal lenses), is when we resort to monovision. Through new lasers and the latest generation of intraocular lenses, we can take advantage of the physiological difference of approaches we have seen before and enhance an eye for far and non-dominant vision for near vision.
Monovision is not something new, this was done years ago but the results were not entirely good, it was necessary to leave a high graduation difference between the two eyes so that it could be seen well from far and close, but this difference was so great that many times patients did not adapt at all well and also lost stereopsis or relief vision.
Monovision today
Currently the situation is very different and we talk about “Blended-Monovision" or "Micro-Monovison", Since the new optical profiles, allow us to get a good view from far and near with a minimum change of graduation.
By using hyperprolate aspherical profiles in corneal cutting with the laser or those same profiles in intraocular lenses, we can achieve that the dominant eye has a very good distance and intermediate vision and somewhat less near. In the non-dominant eye, we enhance near and intermediate vision and somewhat less distance vision, thus, with both eyes simultaneously, we can see very well at all distances, without adaptation discomfort and without losing the ability to stereopsis.
In the figures we see how a hyperprolate profile works, basically consists in the power of the lens changes from the center to the periphery, more power in the center, for the near vision and less towards the periphery, for far, without sudden changes and without needing to look for the focus area as it happens in glasses with progressive lenses.
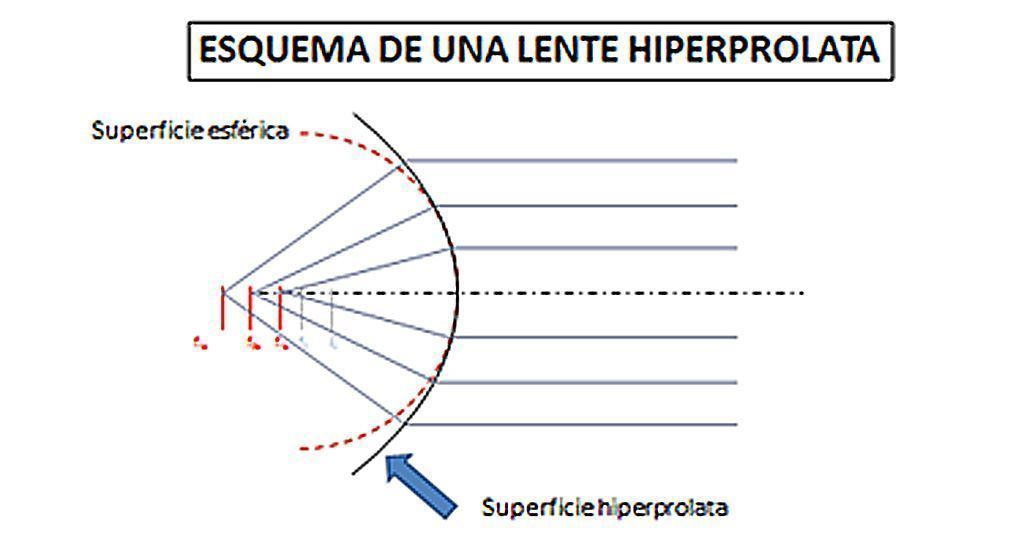
The rays of light that cross a hyperprolate surface converge in different foci, the paracentral ones have the furthest focus and the central rays, have the closest focus, as if the power of that surface increases, such as occurs in the eye when, it passes to focus from far to near. It increases its dioptric power.

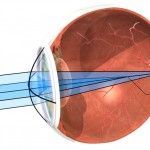
The hyperprolate cornea (arrow), concentrates the paracentral rays of light in a focus located in the retina, in the macula.
When looking at each other closely, close the iris (myosis) and only light rays pass through the cornea in its central area, where the hyperprolatory cornea we have cut with the laser is more powerful, we get nearby objects to focus on the macula.

What should we do to make the monovision successful?
The first thing to do is see the stereopsis ability of the patient, even in cases of Cataracts, you can make an approach that will help us in making decisions. Second, we must study the possibility of implanting multifocal lenses that correct far-near equally in both eyes, with which monovision will no longer be necessary. If this is not the case, then monovision is indicated and we move on to the third point, to study if we perform a corneal laser or indicate an intraocular lens. The differential fact is in how the lens is, if it is okay we can do laser treatment and in case it starts changes towards the cataract or when it is already established, we will go to implant an intraocular lens.
In cases where there are no cataracts, a stereopsis study and a simulation of the situation that will be obtained after surgery can be done. It is not perfect but this type of study allows us to see if the patient will have a good tolerance and a correct vision, preserving a sufficient degree of stereopsis that allows him to continue seeing in relief and calculating the distances well, key in activities such as driving.
Who should perform these types of interventions?
It will always be the ophthalmologist, with his team of optometrists, who studies each patient and decides the best indication. They should go to a Center with experience in visual recovery, where they are used to assessing all the factors that we have mentioned, that have the capacity to study the condition of the eyes, the ametropia they suffer, the condition of the lens, that there are no other diseases , systemic or ocular, that could influence the result and that have the means to study monocular, binocular and stereoscopic vision, to decide the degree of monovision and ocular dominance.
With all these requirements, we can say that the monovision, in its current form, the "Micro-monovision", remains a valid option to solve the problem of glasses far and near, without forgetting the intermediate vision.